
Benign Paroxysmal Positional Vertigo is also referred to as BPPV. A BPPV diagnosis can be extremely unpleasant, however, BPPV treatment is usually very successful.
BPPV symptoms usually occur with particular movements, such as; rolling over or sitting up in bed, bending to pick up an object off the floor or hanging the washing on the line. The attacks are classically sudden and violent and typically last for about half a minute but can leave you feeling ‘off balance’ for quite some time. Several vertigo exercises can provide relief from these BPPV symptoms.
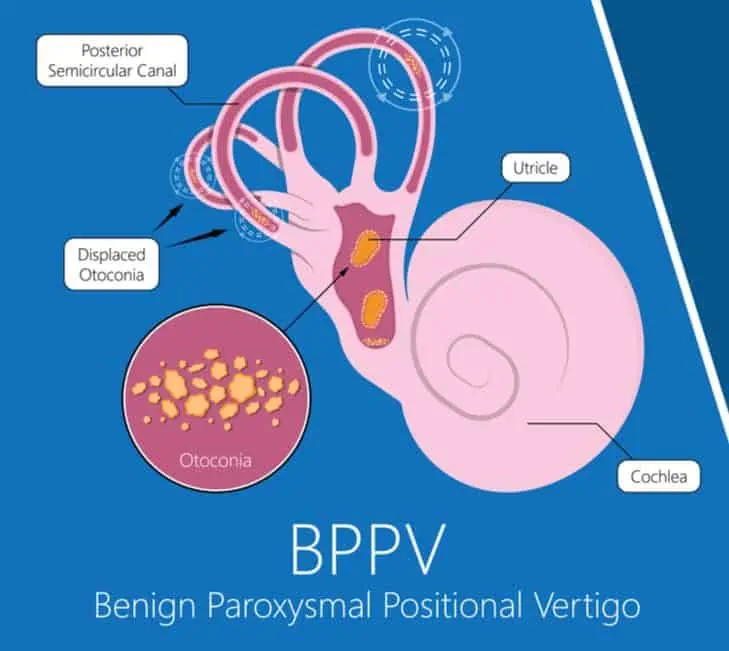
Benign Positional Vertigo occurs when otoconia (tiny calcium carbonate ear crystals, like grains of sand – which are normally found in the balance organ) dislodge and migrate into the semicircular canals. The cause of positional vertigo, specifically BPPV, is most often unknown or idiopathic.
However, there is evidence that BPPV can develop secondary to an inner ear disease (such as vestibular neuronitis, labyrinthitis or Ménière’s disease). The likelihood of onset is known to increase with age.
Head trauma can cause BPPV, and evidence suggests that hormonal factors can affect BPPV, with a significant association between benign positional vertigo and osteopenia/osteoporosis.
BPPV Symptoms
Changes in head position alter the orientation of the semicircular canals, and gravity causes the dislodged ear crystals to shift, stimulating the balance system and causing brief symptoms of BPPV.
BPPV most commonly affects the posterior semicircular canal, but the horizontal and anterior canals can also be affected. The affected canal will determine the sorts of movements that will trigger the dizziness and the direction of spinning sensations that the BPPV sufferer will experience.
There are two types of BPPV. The most common type is canalithiasis, in which the ear crystals are free-floating within the fluid in the semicircular canal. When there is a change in canal orientation, the ear crystals float downwards, stimulating the balance organ as they go. The ear crystals settle at the bottom of the canal within a few seconds, and the BPPV symptoms will stop.
The second, much rarer type is cupulolithiasis. In this type of BPPV, the crystals become fixed within the canal. Dizziness, in this case, can be slower to onset and may last for an extended time.
BPPV Prevalence
Benign Positional Vertigo has a lifetime prevalence of 2.4%. It is more common in women than men. BPPV symptoms are also more prevalent in the elderly than in younger populations.
Posterior canal BPPV is the most common, accounting for between 60 and 90% of cases.
Horizontal canal BPPV accounts for between 5 – 30% of cases, and the remainder is comprised of anterior canal BPPV and multiple canal BPPV.
BPPV Diagnosis
Positional vertigo is diagnosed with the use of positioning manoeuvres which aim to evoke the BPPV symptoms and record eye movements while it is occurring. By combining information about the activity that elicits the response and eye movement direction, the specialist can establish which canal the ear crystals are in.
BPPV Treatment
BPPV will often spontaneously resolve as the otoconia naturally move around the semicircular canal and they may naturally exit the affected semicircular canal. If the benign positional vertigo is persistent, treatment may be administered.
BPPV treatment is aimed at moving the ear crystals out of the semicircular canal using a repositioning manoeuvre that should initially be performed by a medical practitioner, vestibular physiotherapist or vestibular audiologist. The repositioning manoeuvre that is used will be determined by which canal is affected and which type of BPPV the client has.
Often following the repositioning manoeuvre and associated vertigo exercises, it is necessary to sleep in a particular way, to prevent the otoconia from moving back. Repositioning manoeuvres is often successful after just one treatment, but multiple treatments and BPPV exercises may be required in some circumstances.
Often vertigo exercises will be given that can be used at home if the first treatment does not work.
There are rare instances when BPPV does not respond to treatment or vertigo exercises. In these cases (referred to as intractable BPPV), surgical treatment may be recommended. Surgical options are discussed and decided upon with an Ear, Nose and Throat (ENT) specialist.
Your ENT specialist can advise of the risks of such a procedure.
BPPV Recurrence
Just as the otoconia can be shifted out of the semicircular canals, it is possible that they can find their way back, either to the same canal or to a different canal. Studies have shown that around a quarter of people who are having success with BPPV treatment can have a recurrence. Treatment options are the same for subsequent bouts of BPPV as they are for the initial episode.