Tinnitus affects over 60% of your patients.2 Understanding the impact on overall health and social well-being, is critical for providing whole-person healthcare that considers physical, psychological, and social aspects.
Sasha Benatar
Senior Audiologist and Tinnitus Specialist
Lions Hearing Clinic
Tinnitus is a diverse condition that often presents as a ringing, buzzing, roaring, hissing or whooshing like sound. Of most concern is tinnitus often coexists with mental health conditions, including anxiety and depression, and causes a psychological burden to the affected individual.5
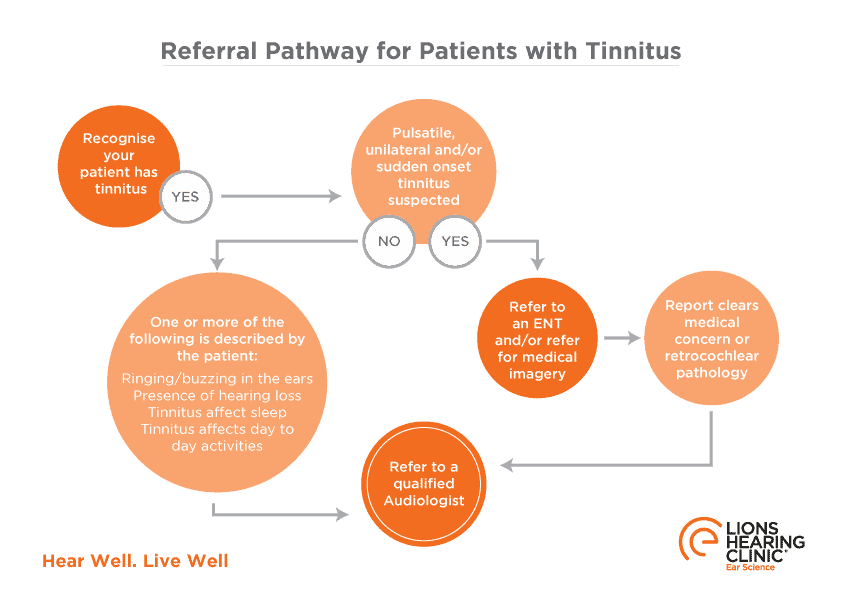
The first step to managing tinnitus is positive reinforcement from a general practitioner and referral for a comprehensive tinnitus assessment.
What is Tinnitus?
Tinnitus is not a disease, rather a symptom of an underlying condition.4 Tinnitus is defined as the conscious awareness of a sound in the absence of an external sound source.1
“Even moderate tinnitus can impact on work and social relationships”
Tinnitus may be present in one (unilateral) or both ears (bilateral) or centrally in the head. It may be continuous or intermittent, with onset acute (< six months) or chronic (≥ six months).
Tinnitus is prevalent amongst the Australian population, with two in three Australians experiencing tinnitus at some point in their lives and one in ten to one in five experiencing severe tinnitus, which significantly impacts on quality of life.2
Tinnitus can occur at any age; however, the incidence rate increases with age, peaking between 60-69 years of age.3
Tinnitus is classified into two types. 4
- The most common form of tinnitus is Subjective Tinnitus, which is the perception of sound heard only by the affected individual.
- The less common form, Objective Tinnitus occurs when tinnitus is audible to the affected individual and by an external observer (e.g. a physician).4 Objective tinnitus may be referred to as a Somatosound, generated from structures near the ear manifesting as either pulse-synchronous (e.g. vascular or respiratory) or pulse-asynchronous (e.g. muscular).
How to Recognise the Symptoms of Tinnitus?
Tinnitus is commonly described as a ringing, buzzing, roaring, hissing or whooshing like sound. Tinnitus often coexists with mental health conditions, including anxiety and depression, and causes a psychological burden to the affected individual.5
Patients may report concentration difficulties, sleep disturbance, effects on relationships and situational avoidance behaviours.
In severe cases, a patient may experience suicidal ideations.7
What Causes Tinnitus?
Due to its heterogeneous nature, there is no single identifiable cause. A well-recognised risk factor is hearing loss.
A widely accepted theory suggests tinnitus may result from cochlea hair cell (cilia) damage and conscious awareness of spontaneous electrical activity. Sensorineural hearing loss is the most common form of hearing loss due to irreversible cilia damage. The lack of external stimulation causes the brain to search for sound internally, altering sensory gating mechanisms and increasing conscious awareness of spontaneous electrical activity. These sounds are usually safely ignored and ‘filtered out’. This unfamiliar activity may be labelled tinnitus and deemed threatening. The brain then begins paying increased attention and engages the limbic and autonomic nervous systems. Thus, in some cases, leading to heightened levels of annoyance and associated distress.4
“Hearing loss is a known cause of tinnitus & can be managed”
Audiological Management of Tinnitus
At Lions Hearing Clinic, we work within a multi-disciplinary team to manage tinnitus. We utilise evidence-based management strategies which decrease a patient’s negative perception, thus reducing the impact on their quality of life. Management is tailored to a patient’s needs with the overall goal to promote habituation, explained as a state of mind where an individual no longer has a negative emotional response to tinnitus.
“Habituation can help the brain tune out the tinnitus.”
At an audiological tinnitus assessment, the patient will complete a tinnitus questionnaire, like the Tinnitus Functional Index, associated history form and work through an extensive case history with the Audiologist. These subjective measures provide the audiologist insight into the physiological impact of tinnitus and information relating to onset, localisation and effect on quality of life.
The Audiologist guides the patient through a comprehensive hearing assessment and includes measurements to quantify the tinnitus perceived, namely pitch and loudness matching. The assessment results are explained, including what may be contributing to the perpetuation of tinnitus distress.
The final element is education which is essential in tinnitus management. Empowering clients with skills to modify their negative thought patterns and adjust behaviours that reinforce troublesome tinnitus, providing a sense of control.
“The first step to treating & managing tinnitus is positive reinforcement”
Common Management Options
Hearing Aids | Recommended when the patient has a hearing loss and experiences tinnitus distress. Hearing aids reduce the strain required to ‘hear’ and increase environmental sound stimulation, which may decrease the perception of tinnitus.
Sound Enrichment/Sound Therapy | These tools reduce the contrast between tinnitus and silence, making the tinnitus is less ‘obvious’, helping the brain to pay less attention to it.
Cognitive Behavioural Therapy (CBT) | The limbic system is closely associated with tinnitus distress.3 CBT is part of a holistic approach to management, facilitating cognitive restructuring to address the patient’s negative emotions that reinforce the perpetuation of tinnitus as an alarm signal. 4, 6
When to Treat Tinnitus with Medical Urgency?
If your patient presents with sudden onset tinnitus and associated sudden loss of hearing, it may be an idiopathic sudden sensorineural hearing loss. Prompt intervention and medical treatment improve recovery and overall outcome.9
When a patient presents with pulsatile tinnitus (pulse-synchronous with their heartbeat), medical investigation by Ear Nose and Throat (ENT) specialist is warranted.
If your patient is experiencing suicidal thoughts or significant emotional distress, refer for emergency help.
The role of an Audiologist in your patient care
For all non-medically concerning tinnitus, the most efficient pathway is a referral to an Audiologist.
Ear Science Institute Australia promotes an evidence-based, whole-person approach to clinical care. Lions Hearing Clinic draws on a team of specialists, including ENTs and Psychologists, to effectively manage the impact of tinnitus. The individual patient’s needs will guide the management approach to reduce the negative emotional response to tinnitus.
CONTACT THE HEARING & TINNITUS ADVICE LINE NOW
References: 1) https://www.tinnitus.org.uk/ 2) HealthDirect. (2021). Tinnitus. Healthdirect.gov.au, from https://www.healthdirect.gov.au/tinnitus. 3) Wu, V., Cooke, B., Eitutis, S., Simpson, M., & Beyea, J. A. (2018). Approach to tinnitus management. Canadian family physician Medecin de famille canadien, 64(7), 491–495. 4) Han BI, Lee HW, Kim TY, Lim JS, Shin KS. Tinnitus: characteristics, causes, mechanisms, and treatments. J Clin Neurol. 2009;5(1):11-19. doi:10.3988/jcn.2009.5.1.11 5) Stegeman, I., Eikelboom, R., Smit, A., Baguley, D., Bucks, R., Stokroos, R., Bennett, R., Tegg-Quinn, S., Hunter, M. and Atlas, M., 2021. Tinnitus and its associations with general health, mental health and hearing loss. Tinnitus - An Interdisciplinary Approach Towards Individualized Treatment: Towards understanding the complexity of tinnitus, [online] pp.431-450. Available at: <https://www.sciencedirect.com/science/article/abs/pii/S0079612321000236?via%3Dihub> [Accessed 17 January 2022]. 6) Atik A. (2014). Pathophysiology and treatment of tinnitus: an elusive disease. Indian journal of otolaryngology and head and neck surgery: official publication of the Association of Otolaryngologists of India, 66(Suppl 1), 1–5. https://doi.org/10.1007/s12070-011-0374-8 7) Han, K. M., Ko, Y. H., Shin, C., Lee, J. H., Choi, J., Kwon, D. Y., Yoon, H. K., Han, C., & Kim, Y. K. (2018). Tinnitus, depression, and suicidal ideation in adults: A nationally representative general population sample. Journal of psychiatric research, 98, 124–132. 8) Leung MA, Flaherty A, Zhang JA, Hara J, Barber W, Burgess L. Sudden Sensorineural Hearing Loss: Primary Care Update. Hawaii J Med Public Health. 2016 Jun;75(6):172-4. PMID: 27413627; PMCID: PMC4928516.





